Butler Center for Research
Women and Alcohol
Butler Center for Research - December 2017

Download the Women and Alcohol Research Update.
With all of the recent attention focused on the opioid crisis, it is easy to overlook the fact that misuse of alcohol continues to be a serious issue for millions of people in the United States. A 2016 survey by SAMHSA revealed that 65 million people age 12 and older engage in binge drinking (consuming five or more drinks during one occasion for men and four or more drinks per occasion for women), and 16 million of those people binge drink five or more times per month. Data on rates of alcohol addiction are equally concerning: an estimated 15.1 million people (5.5% of the population) met the criteria for an alcohol use disorder (AUD) in 2016 (SAMHSA, 2017). Though this rate is down from previous years, it still represents a large number of people.
These statistics are important because heavy drinking is associated with a number of unfavorable consequences. Prolonged heavy drinking can cause chronic and sometimes fatal health conditions like liver disease, heart disease, stroke, bleeding and ulcerations of the GI tract, and cancer (WHO, 2014). Heavy drinking also increases the risk of bodily injury, including accidental death via events like car accidents, drownings and homicides (Cherpitel et al., 2015). The brain is affected as well: heavy alcohol use damages the brain and causes a number of impairments in thought processes like memory and decision making (NIAAA, 2004). Heavy drinkers often have significant impairments in daily life functioning including lost productivity at work and an inability to meet basic social obligations like caring for family and loved ones (CDC, 2016). These problems result in significant costs to the individual and his/her quality of life as well as to society overall. Billions of dollars are spent each year for productivity losses and health care costs for managing alcohol-related conditions (Sacks et al., 2015).
Alcohol Use Among Women
As harmful as excessive drinking is for the average person, women are at even greater risk. Research has shown that the problems associated with drinking, especially the health impacts, are especially pronounced for women. A woman is more likely than a man to harm her health with long-term drinking, even if she drinks less alcohol for a shorter period of time (Holman et al., 1996; Piazza et al., 1989). Some research suggests that women who drink heavily are more at risk than men for alcohol-induced injury (Cherpitel et al., 2015; Sugarman et al., 2009) and accidental death. Women also progress more quickly than men from first using alcohol to developing an addiction, a phenomenon known as telescoping (Hernandez-Avila et al., 2004). Women who drink heavily are more likely than women who do not drink to become victims of interpersonal violence or sexual assault (Foran & O'Leary, 2008). For these reasons, it is extremely important for people to be aware of the risks of excessive alcohol use among women.
Though binge and heavy drinking have decreased over the last several years for men, the rates have increased for women, particularly among older adults. Breslow et al. (2017) examined survey data for alcohol use across a 17-year period (from 1997 to 2014). The prevalence of binge drinking for men age 60 and older remained unchanged whereas binge drinking increased roughly 3.7% each year for age 60+ women. Another study examining changes from 2001/2002 to 2012/2013 found a 58% increase in high-risk drinking among women overall (across all ages) compared to a 15% increase for men (Grant et al., 2017). Frequent binge drinking among teens is decreasing overall, but the decrease in girls has been more gradual than for boys (Jang et al., 2017), such that the gender gap that existed for several decades is closing.
The Hazelden Betty Ford Foundation/HealthyWomen survey
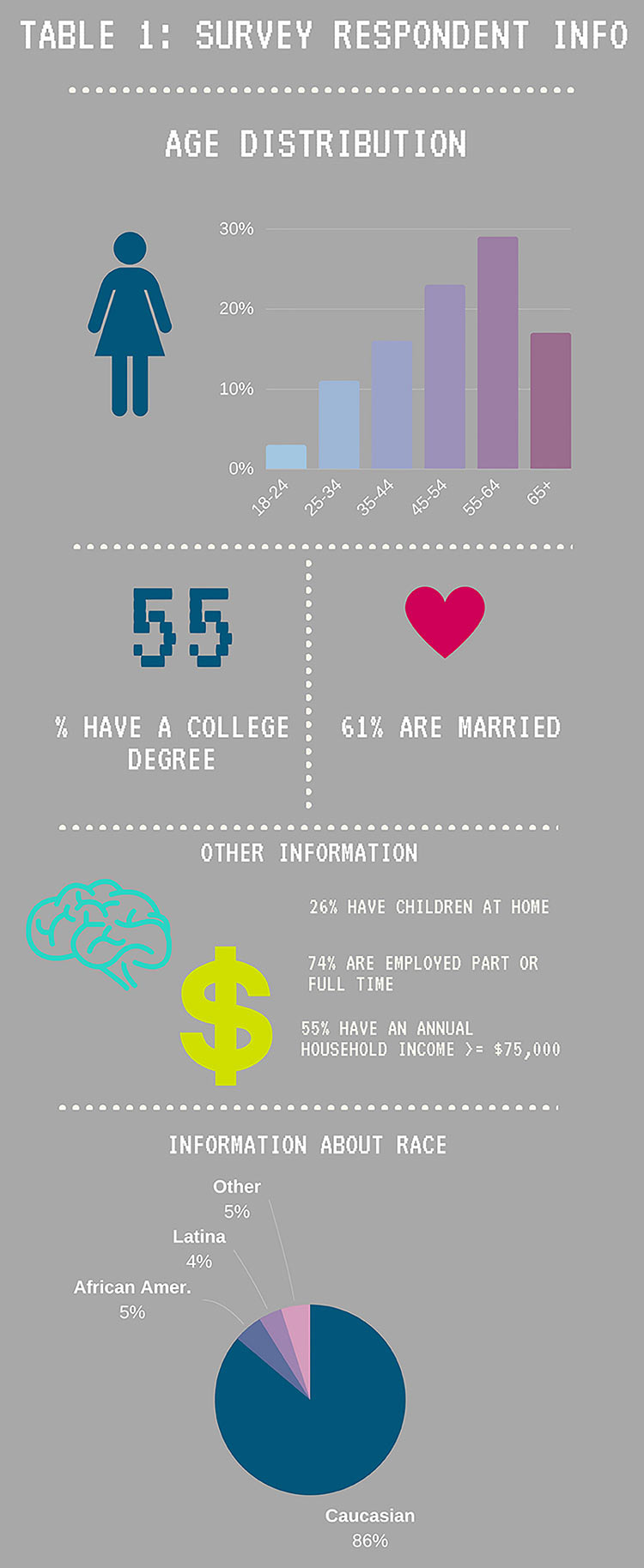
In early 2017, the Hazelden Betty Ford Foundation partnered with the nonprofit organization HealthyWomen to launch an online survey of women's alcohol use. The survey was not administered as part of a scientific study; rather, it was a "pulse" survey to collect current information about how women are drinking, and what beliefs and knowledge they have about heavy drinking. The survey was posted to HealthyWomen.org and advertised on several social media channels inviting women to take the survey. The survey message was: "Do you know the signs of alcohol and drug addiction? You enjoy a drink or two on most days. Could that be the sign of a problem? Please take this brief survey on alcohol and drug addiction." Table 1 (prior page) describes the sample of 1,097 women who completed the survey. They were predominantly Caucasian, older (70% were 45 years or older) and of relatively high socioeconomic status based on annual income, education and job status.
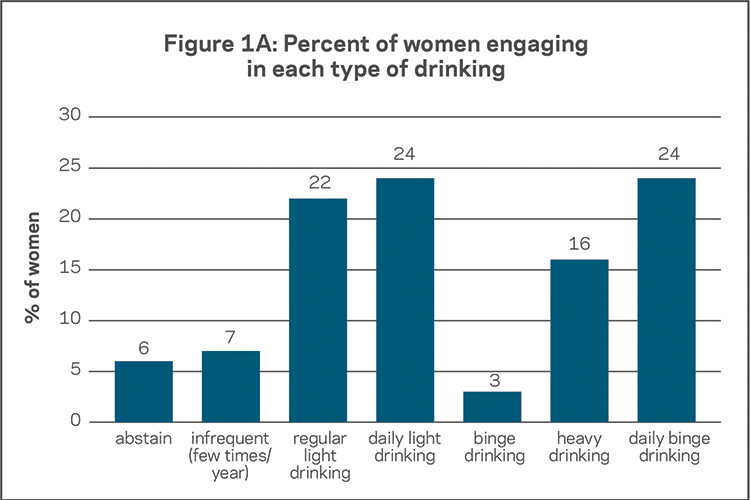
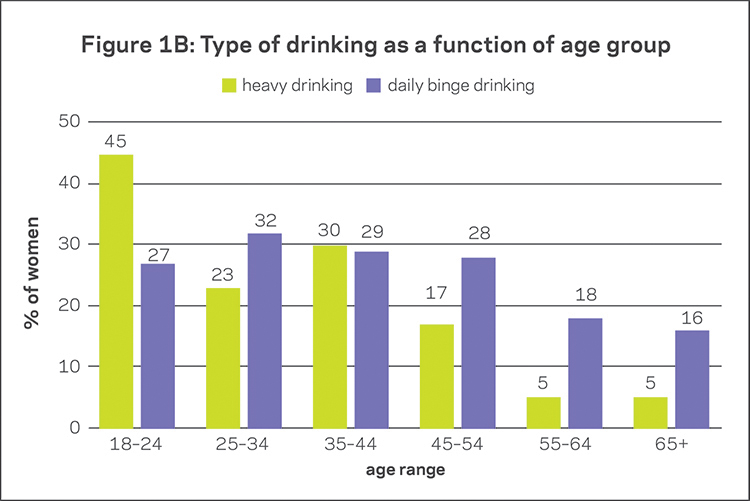
Nearly all women (greater than 95%) answered the demographic questions. In contrast, 402 (just over a third of the sample) skipped all of the alcohol questions. Data on alcohol use therefore came from the 695 women who answered those questions. Key findings are shown in Figure 1A. Forty percent of women reported at-risk drinking, with 24% reporting daily binge drinking (drinking four or more drinks daily or nearly daily) and another 16% reporting heavy drinking (drinking three or more drinks once or twice per week). Because a range of ages were represented, it was possible to examine whether there were significant age differences in drinking behaviors. Results are shown in Figure 1B: 72% of young women age 18-24 reported hazardous drinking, the highest among all age groups. Significance tests revealed that this rate was considerably different than that for 45-54 year olds (45%), 55-64 year olds (24%), and women over 65 (21%; ps < .05). Other surveys have also found that women in their late teens and early twenties are more likely than older women to engage in heavy drinking and frequent binge drinking (SAMHSA, 2017).
The high rates of heavy drinking reported by survey participants are not surprising, given how the survey was advertised. One would expect women who fill out an alcohol use survey to be more likely than the general population to report heavy and at-risk alcohol use. Another large national survey called NESARC showed that in 2013, 9% of women engaged in high-risk drinking over the past year (Grant et al., 2017). In addition, the 2016 SAMHSA survey reported that only 4% of women age 12 and older engaged in heavy drinking. These results are much lower than those found in the Hazelden Betty Ford Foundation survey. However, the National Health Interview survey (from the CDC) found that 33% of Caucasian women ages 35-54 binge drink (Keating, 2016). Notably, most women who completed the Hazelden Betty Ford Foundation survey were of this race and age range. Regardless of whether heavy drinkers are over-represented in the Hazelden Betty Ford Foundation survey respondents, it is clear that an alarming number of women engage in heavy drinking, which carries significant health and safety risks.
Drinking-Related Beliefs
The survey provided an opportunity to learn more about the thoughts, beliefs and attitudes held by women who drink, including the reasons why they drink. One question about motivations for drinking presented a number of potential reasons, and women were asked to select all that applied to them. Forty-two percent of respondents said they often or always drink to have fun; 23% said they often or always drink to forget problems, 42% said often or always to relieve stress, and 72% said often or always because they enjoy it. These data suggest that in this sample of women, the majority drink to have a good time and enjoy themselves, but some women use alcohol to help cope with negative aspects of their lives (i.e., problems and stress). Another key finding related to drinking beliefs was that 67% of women said that most women they know drink as much or more than they do. This is important given that drinking behavior, especially among young people, can be impacted by a person's views about how much other people drink (Foxcroft et al., 2015). Another finding was an age difference in endorsement of the statement: "It's okay to get drunk as long as it's not every day." The 18-24 year old age group tended to endorse this statement (33% strongly agreed and 5% strongly disagreed) more than women age 65 and older, who showed the opposite pattern of responses (9% strongly agreed and 76% strongly disagreed).
Only 20% of women in the sample agreed to the statement that addiction is completely within a person's control, yet 55% said they would feel embarrassed or ashamed if they had a drinking problem. Thirty percent (nearly one out of three) said people would think less of them if they received addiction treatment, and 53% agreed with the statement that women with alcohol/drug problems are more likely than men to be viewed negatively. These findings as a whole reflect the stigma around having an alcohol problem, and research indicates this stigma is alive and well. Lang & Rosenberg (2017) found that people self-reported not wanting to affiliate with people with an alcohol problem, including as a colleague at work and as a neighbor. In another study, women with alcohol addiction who attended treatment stated they were undeserving of support/help (Gunn & Canada, 2015). Though speculative, it is possible that stigma may be a reason that nearly one-third of women who took the Hazelden Betty Ford Foundation survey did not answer the alcohol questions. It's critical to address and break through stigma, because it can make women less likely to admit they have a problem, thereby preventing them from seeking help (Copeland, 1997; Kulesza et al., 2013).
Beliefs About Addiction Treatment
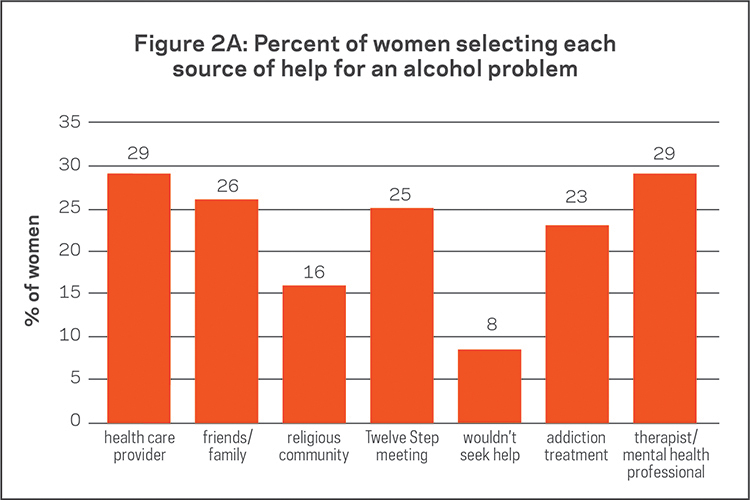
The survey also asked what sources of support women would seek out if they had an alcohol or drug problem; each participant was asked to select all sources that applied to her. Figure 2A shows the percentage who strongly agreed with the source of help when it appeared as a statement (e.g., "I would seek help from a health care provider"). These data suggest that women would seek a variety of sources for help and are consistent with results of past studies, which show that many women with alcohol and drug issues seek help in mental health or primary care settings (Green, 2017). Women reported being just as likely if not more likely to seek addiction treatment in mental health settings (29%) or general health care settings (29%) than in addiction treatment settings (23%). Importantly, only 8% of the women who completed the survey strongly agreed with the statement that they would not seek help and hope the problem goes away on its own.
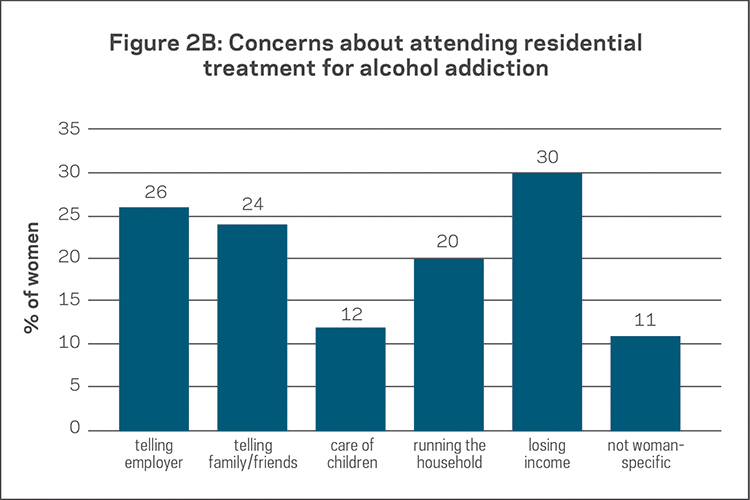
When asked to select the concerns they would have if they needed to go away to residential treatment for alcohol/drug addiction, many reasons were selected (see Figure 2B). The most common concern was a loss of income (30% selected this). Twenty percent of women stated they would be concerned about who would run the household. The responses for income loss and household concerns denote a theme of women worrying about the economic implications of attending treatment. Another theme was being afraid to tell people of importance about attending treatment: telling family/friends and telling one's employer were the second and third most-endorsed barriers to seeking treatment. These findings are consistent with past research and may reflect the strong degree of stigma still surrounding substance use disorders. Lastly, in past studies, responsibility for child care was perceived as a large barrier to attending treatment (Grella, 1997). This most likely was not a large concern for our respondents because very few (26%) reported children living in their household.
It is important to note that many studies have shown a large unmet need for addiction treatment: among an estimated 20 million people in need of treatment for a substance use disorder in 2016, only 2.2 million (11%) received treatment at a specialized facility (SAMHSA, 2016). Of the 20 million people with a substance abuse disorder (SUD), more than 15 million had an AUD. Of these, more than 5.6 million were women (comprising 4.1% of all women in the U.S.) and 9.4 million were men (comprising 7.2% of all men). According to SAMHSA, 806,000 women received AUD treatment in 2016, compared to 1,494,000 men. Based on these data, women with alcohol disorders are attending addiction treatment at specialized facilities at nearly the same rate as men (14.4% vs. 15.9%). This is important because older studies (conducted over 10 years ago) have reported that women are less likely to receive addiction treatment than men (e.g., see Greenfield et al., 2010). Future research should focus more on elucidating the barriers preventing both women and men from accessing health care services for alcohol/drug addiction, so that these barriers can be overcome.
Summary and Conclusions
Millions of women in the United States engage in drinking behavior that poses a substantial risk to their health and well-being, particularly young women in their late teens and early twenties. Women may also face challenges in acknowledging and admitting a drinking problem and in accessing help when they need it. These challenges range from not being aware that their drinking is a problem (i.e., "normalizing" their drinking based on what they perceive others are doing), being afraid to admit to problem-drinking due to societal stigma and worrying about how attending alcohol treatment would disrupt their lives. These barriers are important because evidence shows that once a person is drinking problematically, and becomes physically and psychologically dependent on alcohol, they are unlikely to recover on their own (Moos & Moos, 2006). It is crucial for women to be aware of the risks of heavy drinking and to have access to resources that support healthy drinking or abstinence if that is the best path for them.
The Hazelden Betty Ford Foundation Experience
In the period spanning July 2016 through June 2017, nearly 500 women attended Hazelden Betty Ford's adult residential treatment program in Center City, Minnesota. Staff members of the Butler Center for Research successfully contacted the majority of these women roughly one and three months after residential treatment. Patients were asked a number of questions about their life functioning since leaving treatment, including alcohol and drug use. One month following treatment, 88% of women reported complete abstinence from alcohol and illicit drugs. Seventy-four percent reported complete abstinence three months following treatment. Most of these women were drinking very heavily prior to coming to treatment. At both follow-up points after treatment, these outcomes were similar to those observed for men attending the same program. Outcomes data from other studies are similar to those of the Hazelden Betty Ford Foundation: when people attend treatment for alcohol/drug addiction, many of them do get better (Moos & Moos, 2006; Greenfield et al, 2007). Addiction treatment scientists, including those in the Butler Center for Research, continue to focus on increasing our understanding of why some patients do very well after treatment, while others continue to struggle with substance use.
How to Use This Information
Primary care physicians: It is important to ask each of your patients about their drug and alcohol use, even if it doesn't seem relevant to the health issue they are asking you to treat. Routine medical check-ups and physicals are a missed opportunity to learn about substance use, and provide a quick screen for substance use problems if the patient self-reports using over normal levels.
Mental health therapists: If the patient doesn't self-disclose information about alcohol and drug use, you should ask them. Patients who experience fluctuations in mental health symptoms, particularly anxiety and depression, sometimes use alcohol and drugs in unhealthy amounts. If a patient does have a substance use disorder, treatment should focus on both mental health concerns and substance use, as treating both at the same time results in better long-term outcomes (NIDA, 2010).
